As I’ve mentioned previously, I’ve been reading roughly 10 pages a day of Giovanni Boccaccio’s Decameron as one way of keeping time during the shutdown here in New York City. (Given that my copy is only 562 pages long, but that it took Wuhan 76 days to re-open, I’ve now grown lax with myself about missing a day of reading here or there.) The Decameron is truly a book for our time though. Set against the backdrop of the devastation wrought by the Plague in Florence, it is largely made up of one hundred short stories (ten stories told per day over the course of ten days by ten rich young people who have decamped together from Florence for one after another of their lavish country estates), and although I picked up my used copy years ago – I think from the crunchy old Left Bank Books on Hudson – out of interest in Boccaccio’s famous opening pages, which proceed roughly in the following fashion:
In the year 1348 after the fruitful incarnation of the Son of God, that most beautiful of Italian cities, noble Florence, was attacked by deadly plague. It started in the East either through the influence of heavenly bodies or because God’s just anger with our wicked deeds sent it as a punishment to mortal men [sic]; and in a few years killed an innumerable quantity of people.
The book itself deals vanishingly little with the Plague – preferring, as do its young protagonist, to tell tales of adultery, intrigue, adventure, outrage, hijinks, mistaken identity, and all the rest – which make passing references on page 316 (“The Bishop saw a young woman, who has since died in the present plague…”) and page 335 (“You know that owing to the misery of the times, the judges have deserted the tribunals, the laws both human and divine are silent, and full license is granted everyone to save his [sic] own life.”) the more startling. Fittingly, it is a book which trembles in the nascent fiction of a certain canon between the Medievalism of Chaucer and Dante, and the rambunctious, semi-secular modernity of Rabelais, Cervantes, and Shakespeare.
Now – in our ailing condition of late-capitalist hypermodernity – thank goodness, at least that our current pandemic hasn’t led to quite the degree of suffering and collapse brought on by the Plague that ended Europe’s Middle Ages. Still, we can hope for endings and new beginnings from the global ravages wrought by this novel coronavirus as well.
In recent weeks, I’ve revisited the impacts of and responses to the first cholera epidemic in New York City (1832) and the last great flu pandemic, which hit New York in 1918. Yesterday’s post centered a remarkable chart from NYC’s Department of Health and Mental Hygiene, showing the annual mortality rate for the City from 1800 through 2017 – a few striking key takeaways included: Beyond yellow fever, smallpox, and all other infectious diseases, cholera was far and away the great epidemic killer in New York in the 19th century; after the creation of the Board of Health in 1866, and especially following the introduction of targeted public health interventions (based on breakthroughs in scientific medicine) starting around 1890, the annual death rate in New York City declined drastically from a baseline of around 25 deaths per 1,000 residents to a rate of ~10 deaths per 1,000 which held steady through much of the 20th century; and – although each horrific in its own way – the flu pandemic of 1918-1920, the Great Depression, NYC’s 1970s fiscal crisis, the AIDS Crisis, and September 11th all did comparably little to increase the annual death rate (until the onset of COVID-19, below 6 per 1,000 residents) relative to the staggering progress attributable to the public health advances of the late 19th and early 20th centuries.
So what were those advances? Glad you ask. I’ve leaned heavily on the work of eminent New York City historian Mike Wallace (and his late collaborator, Edwin G. Burrows) and, one last time, will do so again today. Rather than focusing on a particular disease/outbreak this go-around, however, I’m going to revisit, with some brief comments, some of those advances as outlined by Wallace (from page 544 to 560) of his incomparable Greater Gotham. With no further ado:
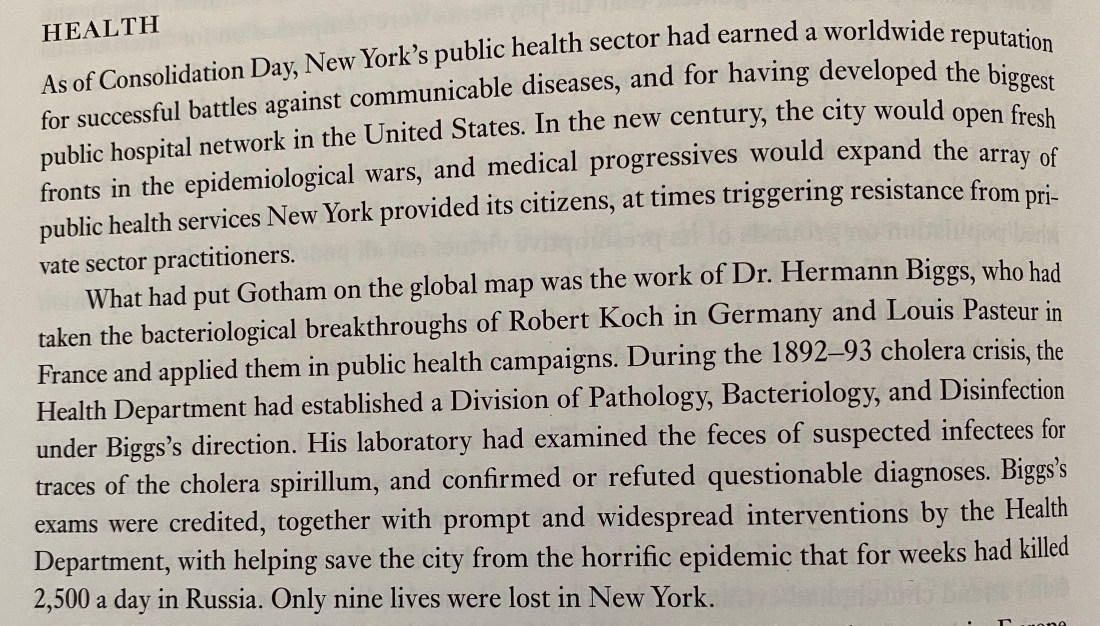
Louis Pasteur and Robert Koch were towering figures in the early history of scientific medicine, and it’s a shame that figures like Dr. Herman Biggs are not more widely remembered and celebrated for their transformative work in New York City. As yesterday’s post highlights, cholera was the great epidemic killer of New Yorkers in the 19th century (for context, no other disease caused the annual mortality rate to spike much above 30 deaths per 1,000 residents; on three separate occasions, cholera epidemics led to spikes in the death rate to ~50 deaths per 1,000, which is to say, 5% of the City’s entire population dying in a single year), and yet, we see above that the work of Dr. Biggs stopped cholera in its deadly tracks; in fact, after 1893, cholera would never again appear in epidemic form in New York City.

So thoroughly do we take these facts for granted, that we tend to be rather shocked and outraged when water and food are not “clean” in New York City today, though, of course, there is both a class component to this expectation (as recent revelations about widespread water system-related lead poisoning across the United States make clear) and a growing threat from our industrial food system and the petro-agro-chemical complex to the safety of our food and water supplies (as evidenced by regular national outbreaks of salmonella, E. coli, etc. and by the increasing prevalence of herbicides, pesticides, and “forever chemicals” in water supplies across the country).
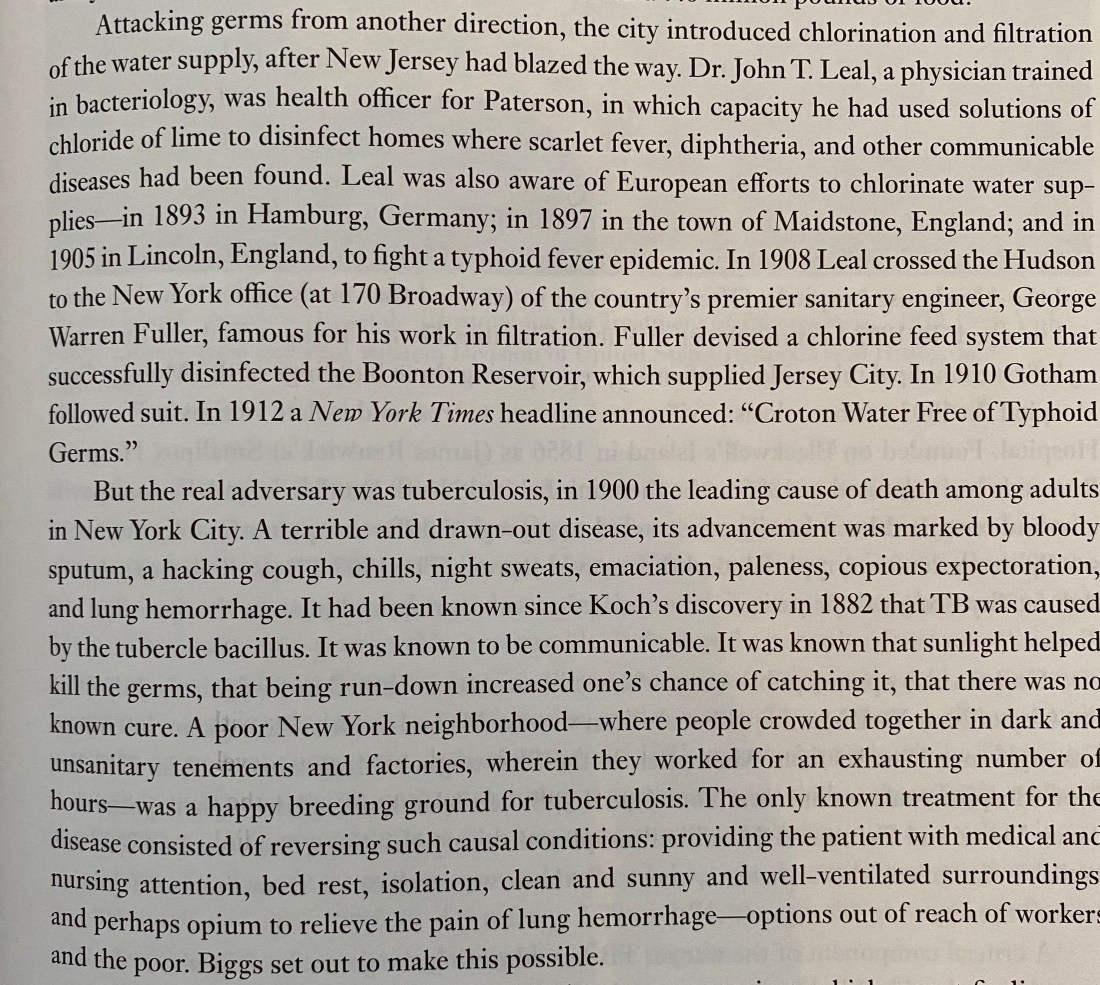
I’ve written elsewhere that anti-vaccine sentiment is only possible in a post-vaccine world (logically, perhaps, but also owing to the privilege of a population that no longer lives in fear of many deadly diseases) and that “conquest” of diseases like tuberculosis in the rich countries allows most people in the United States to ignore the fact that tuberculosis is still the leading infectious cause of death globally. Similarly, while there are valid criticisms of chlorination of water supplies, I’d argue they should always start by affirming the inviolability of access to clean water for all.

This one speaks for itself. As a friend in Bombay wrote yesterday, with some exasperation, regarding the effective response to COVID-19 in the (communist-led) South Indian state of Kerala, “I don’t know why we behave like it’s so tough to do that in India.”
She’s exactly right. Approaches to problems like those we face today in the US, in India, and across much of the world were worked out more than a century ago, and continue to prove effective at present – as has been amply documented and pointed out – in places like South Korea, Taiwan, Singapore, and Hong Kong.

Again, mostly self-evident, though I’ll note that, in New York in the early 19th century, as in New York today, women were often at the forefront of care work and the implementation of sane, holistic models for health.
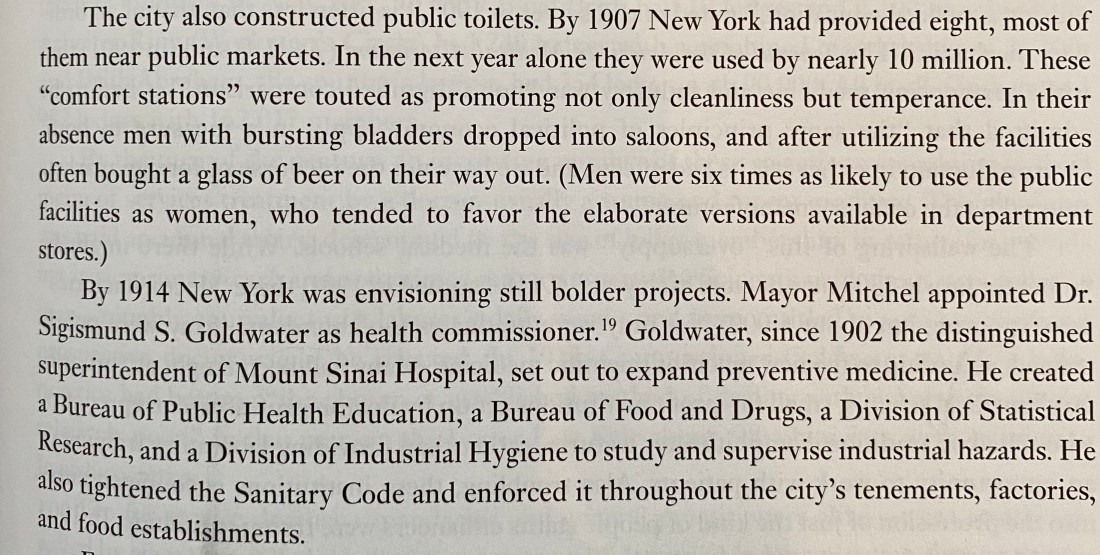
The more things change, the more they stay the same. The (public) money we spend (collectively) on good, clean, well-maintained public toilets yields returns multiple fold over in the form of urban cleanliness, public hygiene, and the peace of mind from which we all benefit in living in a humane society.

For readers interested in a dry, very-deep, but illuminating dive into the struggle between private medicine and public health in the United States, I recommend Paul Starr’s The Social Transformation of American Medicine which I read in college under the guidance of the cantankerous, good-hearted, now-late Joel Schwartz, a model of humane thinking if ever there was one.

“The sea change,” in question was the Flexner Report of 1910 that led to a complete overhaul of medical education and licensing in the US, and the publication of which marked a watershed moment in the establishment of the prestige and power of the medical profession in this country.

This selection is notable for the light it sheds on early corporate consolidation, shifting class dynamics, and gendered labor relative to New York City’s major hospital networks which – consolidations notwithstanding – remain largely unchanged from more than a century ago.

The reactionary power of the private medical establishment has done a great deal to undermine public health in the United States. No clearer example of this fact can be found than in the short paragraphs above starting, “Doctors fought,” “Doctors opposed,” and “Doctors denounced”; incidentally, NYC doctors also fought to prevent the implementation of widespread diphtheria inoculation, then, when it proved effective, fought to prevent this inoculation from being provided free/at low cost as a public good, claiming this would undercut the profits of private medical practitioners.
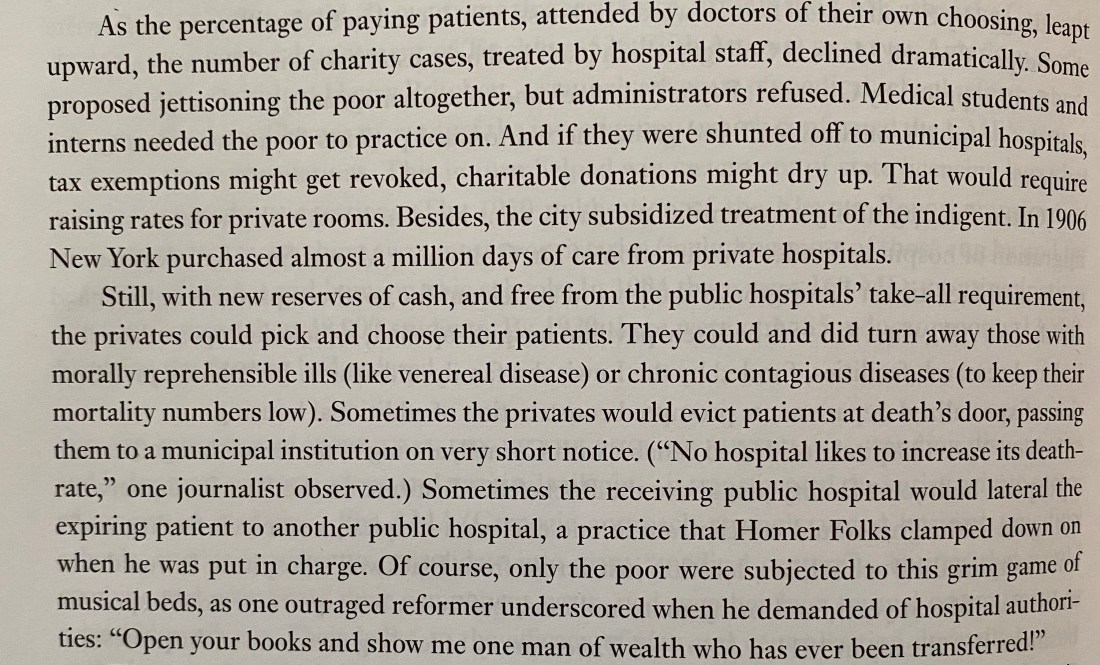
Wallace’s observation that “Medical students and interns needed the poor to practice on,” reflects a long, shameful, often racialized tradition in US medicine that has been amply documented by Harriet Washington, and evidence of which can be found in the sadistic work of J. Marion Sims – “the father of modern gynecology” – of whom the statue was, at last, removed from Central Park not so long ago. The testing of the birth control pill on poor women in Puerto Rico, and the recent proposal by a French scientist to test potential COVID-19 vaccines on the poor in Africa both reflect this same callous spirit evinced by privileged researchers for the lives of others.
As I wrote yesterday, “we, in settler-colonial New York City, are at once descendants – or at least inheritors – of a grisly legacy of violence, and beneficiaries of an almost unimaginable history of progress.”
As we chart our way out of this mess, we should be looking to the lessons of the past to shape a better future. We’ve come a long way, have a long way to go, and have both the benefit of lessons – good and bad – from which to learn and the resources and understanding to do so much more than is currently being done in the name of justice, sanity, and public luxury.

4 thoughts on “When the City Breathes Again, I’ll Breathe Again, Too”