I’m sitting here with our kitchen window cracked open, a slightly too-cool breeze blowing in (I’ve closed the window, but it was nice to feel the air), and still, I can hear a bird I don’t recognize singing, see a person I don’t know going for a jog on her building’s roof – back and forth, back and forth – see the magnolia tree in the courtyard in bloom earlier than I can ever before recall seeing its purple-white flowers.
Yesterday, I delved into the doubts and uncertainties in our knowledge about COVID-19 and SARS-CoV-2 (the virus that causes it). Unsurprisingly, given that it’s a new pathogen and most of the world was – unjustifiably – caught off guard by its emergence, there’s a lot we don’t know. At the same time, as I’ve addressed on many occasions in the past, the root question we should be asking ourselves is: What type of society is it in which we’d like to live? And a follow-up on that: How in the world did we let things get to this point?
My concern – in looking to people of good faith and sound reason who raise valid questions about both our knowledge of and responses to the pandemic – is that the doubts they raise can all too easily serve as fodder for those with more cynical interests – people like our President, or Brazil’s, and the craven politicians of various parties who follow these men. As Adam Serwer of The Atlantic put it on the latest episode of Mehdi Hasan’s brilliant podcast, Deconstructed (an episode the title of which questions if the President’s “Cult” is a “Death Cult,” a question to which I’d have to answer: Yes), in addressing recent brave proclamations by (no-doubt-secretly-self-isolating) prominent Far Right figures: “When they say they’re willing to die for the economy, what they mean is that they’re willing to let you die for the economy. That’s what they really mean.”
In New York City, Democracy Now! reports that “[r]efrigerated trucks and tents have been stationed outside some hospitals to hold the bodies of the dead as morgues fill up.” It only gets worse from here, at least for the next few weeks. I encourage anyone who hasn’t yet to watch this interview (from the same DN! episode) with NYC emergency room physician, Doctors Without Borders volunteer, and Ebola-survivor Dr. Craig Spencer. Already, healthcare workers in New York are starting to report Lombardy-like conditions in our hospitals, and, as my own admittedly back-of-the envelope modeling work suggests (see below), we’re only at the beginning of a very large surge in hospitalizations, ICU admissions, and deaths. As Spencer put it: “In a week, we will be Italy.”
Of course, all of this could have been averted. We know that, because some countries have averted the equivalent. Given our negligence here, and the negligence of others elsewhere, it remains to be seen if South Korea, China, Singapore, Hong Kong, Taiwan, and others will be able to continue to suppress the pandemic, but for now, they’ve proven it is possible to, and should we have done our part in the global struggle, their position would be that much more secure.
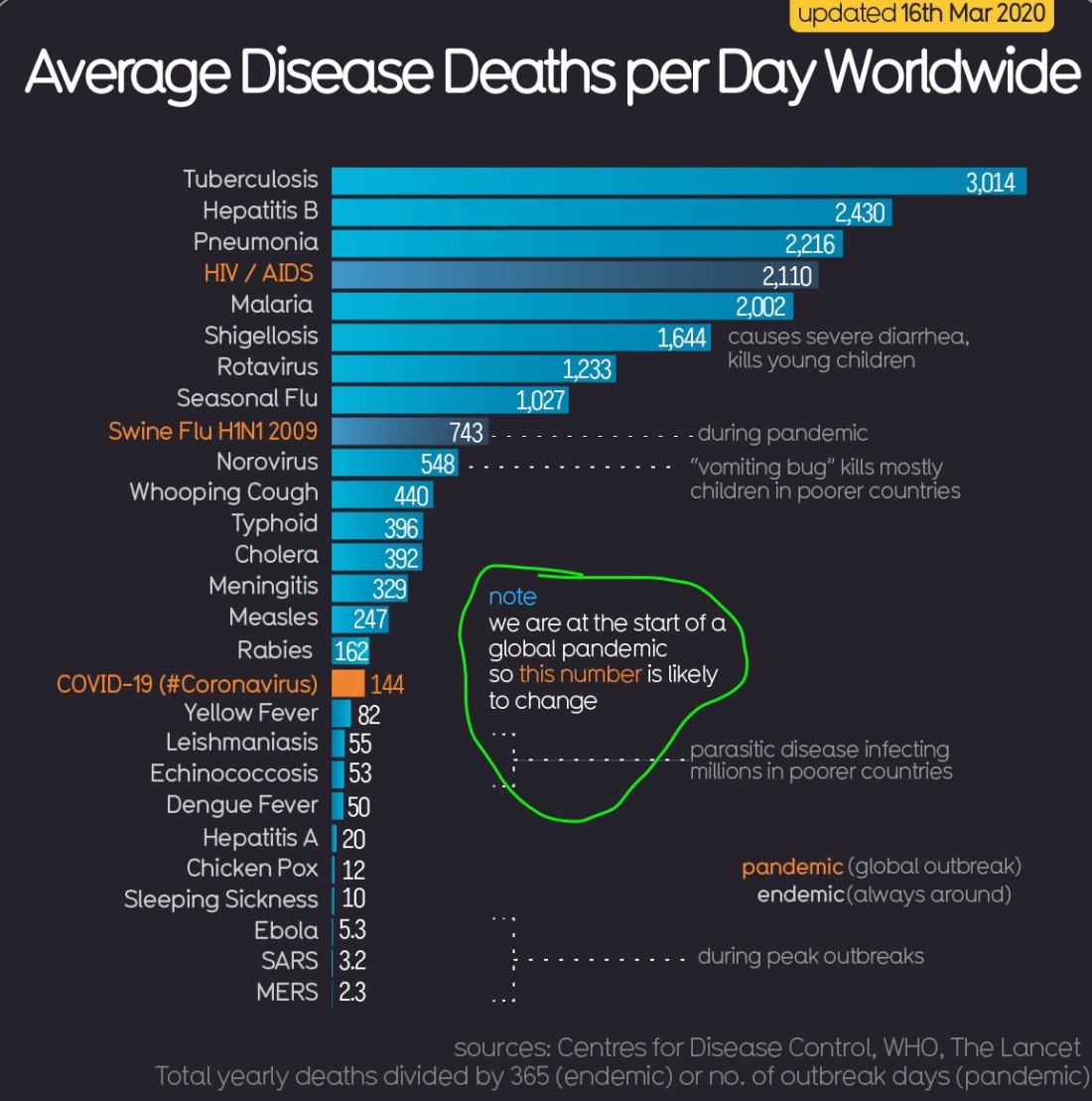
It is also, indeed, possible, that the assumptions I outline in the caption above overstate the deadliness of this disease, but from Italy, Iran, China, and now here in New York City, we have solid, incontrovertible evidence that it is deadly enough. By extrapolating from numbers in Wuhan, or Lombardy – as I attempted to yesterday – we can conclude that this virus is already on pace to kill millions around the world; given the laxity of responses in many places, and the likelihood that we will see second waves of infection in hard hit locales – as lockdown measures are loosened, and owing to the insufficiency of governmental responses and preparation all around the globe – I see it as reasonably likely that it will kill tens of millions.
Speaking of incontrovertible, here’s a graph showing the trend in already confirmed COVID-19 deaths here in NYC.
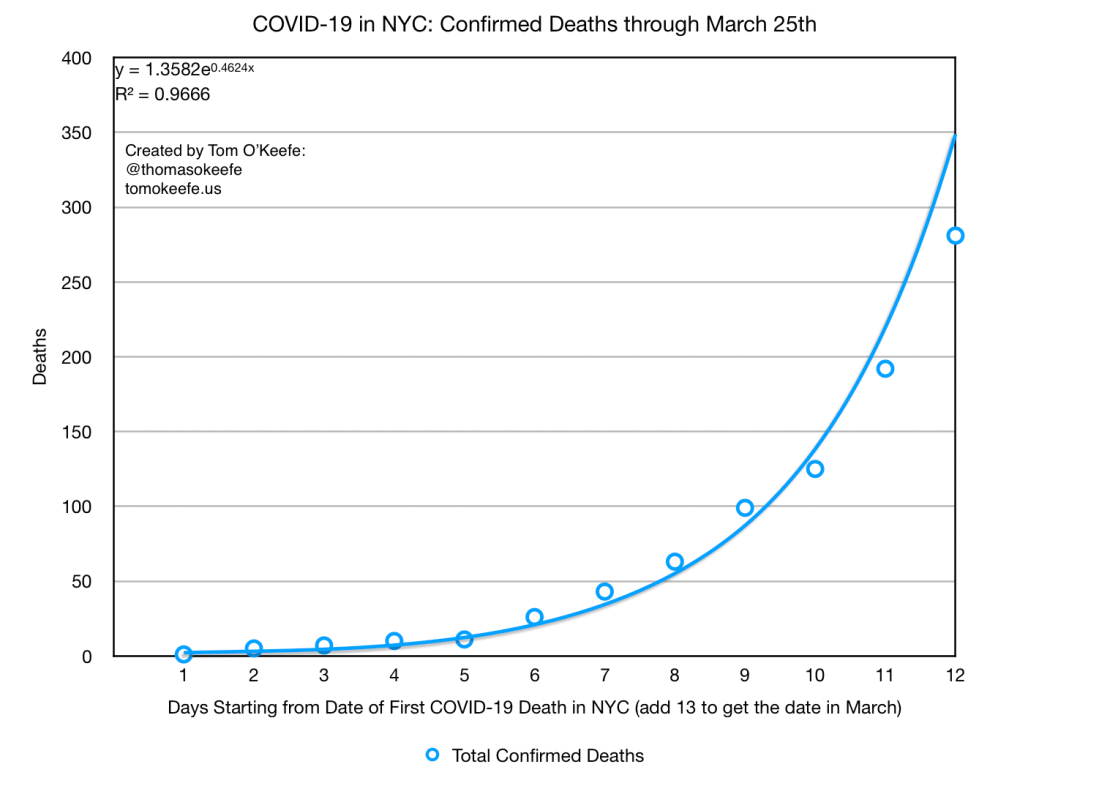
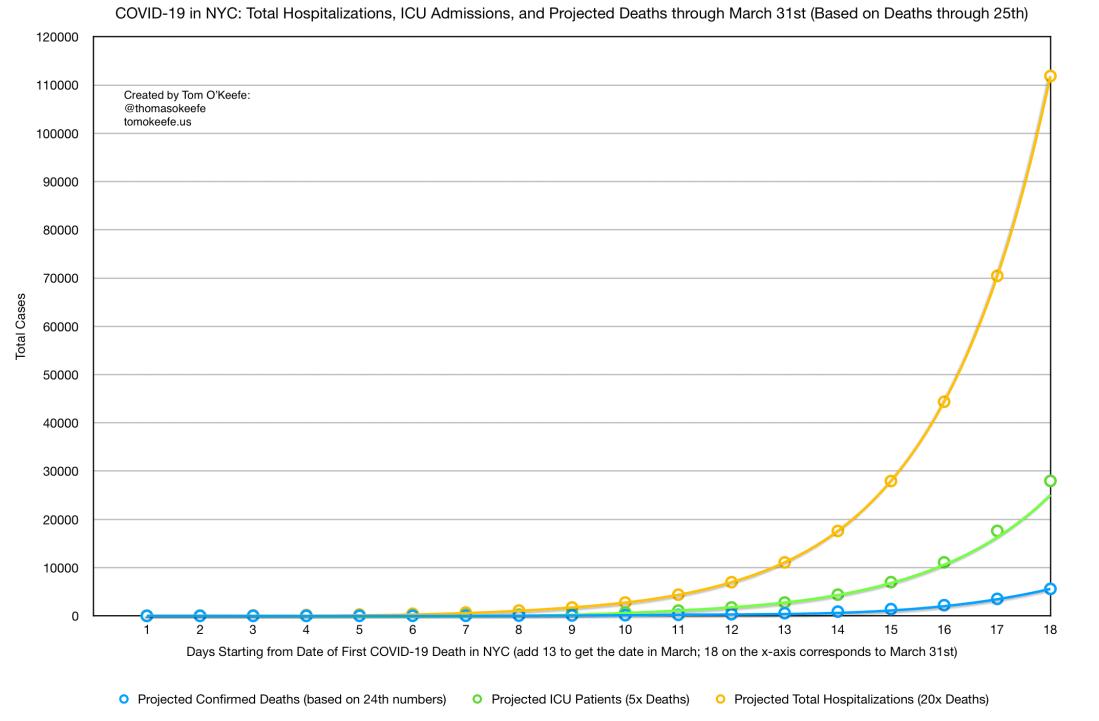
Up until recently, I was still trying to project the total NYC case load based on the confirmed numbers and a model I’d cobbled together based on the data for Wuhan which appeared in JAMA. This week, as the number of deaths has (sadly, predictably) steadily risen, I’ve shifted to the method described in the first caption above.
As you can see below, the projections of number of deaths are starting to converge with ominous implications.

Perhaps most shocking, in a way, though, is what the assumptions outlined in the first caption above suggest regarding the total case load in New York City.

There is truly almost nothing we can do about any of this now – other than respond to it, of course, with humility, compassion, and, at last, due urgency – and the frantic efforts of City, State, Army Corps, and others, to expand our hospital and ICU bed capacity reflects an admirable, if profoundly belated, effort that is likely doomed largely to failure. If the projections are anywhere near correct (you can see that my first graph above calls for more than 100,000 hospitalizations by the end of the month – that is, five or six days from now – and more than 20,000 people requiring ICU care; we have ~20,000 hospital beds and 2,000 ICU beds in the City), our hospitals will be totally overwhelmed, and all we – or really, our healthcare workers and support staffs – can hope to accomplish is harm reduction at the margins of this tragedy.
One form of that to which I’ll point in the spirit of the path forward is the effort which my partner has been pushing forward calling for the urgent creation of alternative birthing sites in NYC. As she argues in her short, powerful piece, Birth Centers NOW:
We have decided that the safest thing for pregnant women to do in this moment is to go into the hospital, the epicenter of our struggle against this disease, while everyone else is asked to shelter in place. Worse — they are induced early (with a significant respiratory risk to neonates), potentially devoid of their partner, family members, their doula, and at significant risks sent home early with nonexistent postpartum care.
She and I have both been working hard on this effort (and making some headway in recent days), and would welcome your support if it speaks to you.
Every day confronts us with reasons for laughter (my mom just sent me this New Yorker piece – first sentence: “Calling it a “promising development,” Dr. Anthony Fauci said on Sunday that alcohol may help people survive the most severe effects of coronavirus briefings.” – and my partner showed me this tremendous Insta post last night); heartbreak (like for the man in Karnataka, in South India, who killed himself for fear he’d contracted the disease); and some combination of the two (as at the inadvertent spread of COVID-19 misinformation by Bollywood legend Amitabh Bachchan); for hope (that “UK researchers develop[ed a] new low-cost, rapid COVID-19 test that could even be used at home”; that people in India, and elsewhere, are finding creative ways to socially distance while still attending to life’s essentials; and that, in spite of lacking our resources, Nigeria may be more prepared (could a country have been less prepared?) than the US to confront the pandemic); and despair (at the behavior of white supremacists on the streets, as in Congress). The DSA has another excellent Bulletin out – which led me to this good piece by Mike Davis on the history and contemporary political economy of pandemics – and Science for the People has issued a well-considered Statement on [the] COVID-19 Pandemic.
The President’s Cabinet has a “Bible Teacher [who] Blames [the] Coronavirus Pandemic on God’s Wrath“; Governor Cuomo (who was in large part responsible for the same hospital cuts that have rendered New York State even less prepared than we would’ve been for this crisis) is now quietly trying to use the confusion of the moment to roll back bail reform; Mayor de Blasio says that half of New Yorkers will likely contract the disease before this is all over (to me, that seems like a conservative estimate, in fact). Bizarrely, the US has chosen this moment to indict President Maduro of Venezuela, and has also recently further ratcheted up its murderous sanctions regime on Iran (and continues its murderous sanctions regime on Cuba), and I hear no reports of talk in Official Washington about reconsideration of the Global War on Terror – the Long War of Cheney, and Rumsfeld, and Wolfowitz – that has wrought so much destruction around the world while siphoning trillions away from essential needs here in the “homeland.”
Still, there’s always good news with the bad: The everyday heroism of New York City doormen – who absolutely shouldn’t be working right now (so this news isn’t especially good, actually); the waiving of monopoly rights to remdesivir by Gilead; the persistent good work of FAIR in holding the corporate media accountable; the steadfast integrity of Tricontinental, in centering the needs of the many over those of the few around the world; and efforts like those of Asian Americans for Equality, to the Emergency Small Business Relief Fund of which I donated this morning.
In what type of society do we want to live? As I write, bodies are piling up in freezer trucks in the parking lots of New York City hospitals. This was an avertible reality, but is now the reality with which we’re stuck. No one is saying – truly no one – that the pandemic response in New York City was flawless, but on the one hand, those who question if we might not have overreacted, I think, increasingly, stand on the wrong side of the facts, and, on the other – frighteningly – our response will likely be much better than the responses of many other places around this country. We have a world-class healthcare system, strong institutions, ample resources, and a long, proud tradition of public health, and still – as I wrote elsewhere some time back – this disease has cut through us like a buzzsaw. Look how quickly New York State ramped up testing, for example. Do you foresee that happening in Mississippi – the governor of which recently declared: “Mississippi’s never going to be China”? And he was right, of course, just not the way he thought he was.
Those of us who believed in commensurate response once the situation had spiraled out of control are, in many instances, the same people who believed in public health all along. To paraphrase something Dr. Spencer said in the above-linked interview, the $2 trillion Congress has just appropriated for pandemic relief – $2 trillion which will likely not be anywhere near enough, especially with so much of it flowing into corporate hands – would have been enough to fund global pandemic preparedness for a decade. The problem was not with the overreaction once the damage was done, but with the inaction for years and decades before; the gutting of essential programs and services; the laying of the groundwork for this global tragedy through what Christian Parenti calls the “catastrophic convergence” of post-Cold War militarism, climate crisis, and capitalism. The work before us is to come up with a life-affirming answer to that question – what type of world? – and to build diligently, for years and decades, towards what that new and better world will be.